Archived Articles 2003
Topics of Interest
- Help keep your workplace healthy in 2003 - Helpful Handouts
- Winter Ergonomics - the Joy of Snow Shovelling
- Ergonomic Hand tools and Modifications
- Help Prevent Aches and Pains on a Long Road Trip
- How to Prepare for an Ergonomics Assessment
- How to Apply Ergonomics Principles to Gardening Tasks
- Put it on Credit!
- Participative Ergonomics
- Radiation Safety and Video Display Terminals (Computer Monitors)
- Work Rest Schedules - A Means of Reducing Musculoskeletal Discomfort in Computer Work
- Ergonomics: Manual Materials Handling
- Prevention of Work Related Upper Extremity Musculoskeletal Disorders
- Children, Computers and Ergonomics - Can they fit together?
- Lateral Epicondylitis (Tennis Elbow): Is There Any Science Out There?
Help keep your workplace healthy in 2003 - Helpful Handouts
Do you want to start 2003 on a pro-active note? Why not provide your employees with information that encourages self-education and ownership into their health and work methods.
One of the more popular New Year resolutions is to get "healthy" or "in shape". This can be an effective goal in the workplace as well. Why not encourage your employees to work in a healthier manner and protect themselves from experiencing an injury. In order to assist you with this, we have collected a number of our reference handouts that some of our clients have found effective. These handouts cover Manual Materials Handling (both during work and leisure activities) and Office Ergonomics, specifically computer based issues.
It is important to understand that these handouts should not replace a full ergonomic assessment or medical treatment but only be used as pro-active education. If someone is currently symptomatic they will require additional attention.
These handouts are in PDF format. If you do not have Adobe Acrobat Reader, click on the icon to download it.

Manual Materials Handling
Safe Manual Materials Handling Tips This handout provides tips and guidance on how to Lift, Push/Pull, and Carry in an ideal manner.
Office Ergonomics
To Top
Winter Ergonomics - the Joy of Snow Shovelling
As winter is here, we should take a moment to remember it can be hard work clearing the snow off our side walks and driveways.
Shovelling in general has been studied in many lab and field studies. Recently there has been an increase in the number of "ergonomically" designed shovels that are available for purchase at the local hardware store. So what this article looks at is, is it worth the extra money to purchase a new shovel? and what should you look for in a good snow shovel?
Snow Shovel Design Facts
The Bent Handle The Liberty Mutual Research Centre for Safety and Health found that when people use a bent shaft snow shovel they bend forward less than with a straight shaft shovel and this may reduced the maximum spinal compressive and shear forces when lifting the loaded shovel from the ground (Hansson and Oberg, 1996)
Metal vs. Plastic Should you go for durability or safety? The trade offs are that a metal shovel is more durable but is the heavier shovel and will result in fatigue faster. A plastic shovel may not last as long but is the lightest material and will be easier to lift.
The Size of the Shovel This, like any other piece of equipment, should match the person doing the shovelling. A taller, heavier person should use a 18" x 16" blade shovel that maximizes the load (covers more area). The shaft should be 52" long with a 1 Ľ" handle. A shorter, lighter person should use a shovel with a blade 16 ˝" x 14 ˝" wide, a shaft 42" long and 1 ˝" handle diameter.
Handles The handles should allow for a free grip when wearing gloves or mittens and cushioned "D" grip handle provides the best grip and comfort. Look for a fibreglass handle if possible. This is up to 3x stronger than wood and won't splinter, warp or dry rot.
Hopefully those facts will help you select the correct shovel for you. After you have the right shovel what else do you need to consider?
Snow Shovelling Tips
- Shovel often - newly fallen snow is lighter than heavily packed snow.
- Push the snow instead of lifting it - where possible, push the snow on the shovel to where you want it.
- If you have to lift the snow:
- Don't bend at the waist, bend at the knees and keep your stomach tight
- Place your hands apart to give extra leverage
- Take small frequent scoops instead of large ones (snow on a shovel can weigh up to 20 lb.)
- Walk to where you want to dump the snow, don't "throw" it
- Don't throw the snow over your shoulder or to the side - this causes twisting
- Pace yourself and take breaks when you feel tired or out of breath
If you enjoy the outdoors, snow shovelling can be a great aerobic activity when done properly. Like any regular exercise you should warm up and stretch before beginning the activity.
However, if you resent this part of winter, the best solution might be a snow blower. If you have a snow blower, there is one main recommendation to ensure you don't over do it. Don't force your snow blower. It is made to work at a certain rate and pushing or forcing it to go faster could result in a back injury.
References:
Quick Tips for Safer Snow Shovelling www.wellnessjunction.com/athome/ergonomics/shovel.htm
Ergonomic Design of the Snow Shovel http://ergo.human.cornell.edu/ErgoPROJECTS/97projects/coffiner.htm
Liberty Mutual - Research Center - Bent -Shaft Snow Shovels Reduce Pressure www.libertymutual.com/research/news/releases/press_snow_shovel.html
To Top
Ergonomic Hand tools and Modifications
(Adapted From: What to look for when selecting or modifying hand tools to provide a better fit with the user, www.arabilityproject.org/assistivetech/tips/handtools.cfm)
In an effort to reduce the ergonomic stress on the upper extremities and reduce the incidence of repetitive strain injury, many companies have started to look at the design of their hand tools. This is often coupled with the desire to create a more efficient tool with better quality output. What they find is that their tools are not ergonomically appropriate and place added force, posture and repetition stress on the body.
Tool developers and ergonomists know that one of the major difficulties in designing the perfect tools lies in the variation in human anthropometry. Additionally, designing a universal tool suitable for all situations is impossible. So what can the tooling engineers, designers and ergonomists due to improve tools? Here are a number of ideas.
All tools should include features that:
- Decrease force or grip strength
- Decrease repetitive motion associated with using the tool
- Decrease awkward postures when using the tool
- Decrease vibration
Factors that can decrease force or applied grip:
- Ensure optimal length and diameter of the tool handle to decrease the force applied.
- Ensure tools with two handles (pliers, scissors) use an optimum grip span suitable for small and large hands, left and right hand operation.
- Investigate coating tools with special material to increase efficiency and reduce the applied forces (i.e. Teflon on saw blade).
- Provide cushion grips to improve comfort, increase slip resistance and reduce the applied grip force.
- Ensure that only personal tools are moulded with finger grips to improve slip resistance. This is a positive feature but you must be sure the tool is only used by the person it was moulded for.
Factors that decrease repetitive motion associated with using the tool:
- Ensure that where possible tools with a ratcheting mechanism or gears are used
- Ensure tools are properly maintained and used properly
- Change to a power tool
- Use tools (pliers, scissors) with adjustable spring loaded returns
- Investigate designs of tools that improve efficiency and reduce the overall repetitiveness.
Factors that decrease awkward postures when using the tool:
- Ensure the appropriate orientation of the handle for the job (pistol grip vs. inline)
- Investigate the use of the bent or curved handled pliers and hammers, which allow the hand to maintain a more neutral wrist position.
Factors that decrease vibration;
- Ensure the tools are maintained regularly to prevent any added vibration due to faulty or worn parts.
- Design power tools with anti-vibration materials or handles
- Investigate using gloves with material that dampens the vibration
If you are not able to implement these factors to make the tool appropriate, then consider changing the process or redistributing the work.
If you are interested in additional tool design guidelines, we have a full Ergonomic Design Guidelines manual available under our Tools section. If you are interested in purchasing one, please send us an email for more details, info@oiweb.com.
To Top
Help Prevent Aches and Pains on a Long Road Trip
In the summer months we tend to hop in the car and go for road trips on a regular basis. When we get to our destination we are often sore and our muscles are tired. In order to try and minimize this, take a couple of minutes and think about each of the following points.
Your Driving Posture
Typically our driving postures are poor. The main areas of concern are with our neck, back and shoulders/ arms.
Neck Posture
The ideal neutral neck posture is when you are sitting with your ear in line with your shoulder, in the vertical plane. You very rarely see people driving in this posture. This is because, many people have their seat reclined too far. If the recline angle is too large, you have to reach to grasp the steering wheel thus you end up rounding your shoulders and bending your neck forward.
Take some time and adjust your mirrors so you can look in them without having to bend your neck forward/ backwards or tilt it to the side.
Back Posture
Back postures and support are also often less than ideal. This is due primarily to how the seat is adjusted. Ideally, you want the seat to be close enough for you to easily fully depress the pedals. The back of the seat should be adjusted so the lumbar pad (bump in the seat back) is located in the curve in your lower back. This will provide support to your lower back muscles and make it easier to sit in the ideal posture.
It is recommended that the seat back be at an angle of between 100 and 110 degrees from the seat pan.
It is also a good idea to remove your wallet or keys from your pockets as they may cause you to sit in awkward postures resulting in uneven stresses on your back.
In some cars the seat back moves forward and backward. If your vehicle has this feature, you should locate the seat back in a position that allows for a 2" - 4" gap between the edge of the seat pan and the back of your knee. This will minimize compression on the back of the knee.
Shoulder Posture
Shoulder and arm fatigue is a common concern when driving for long period of time. This can be true if you have your steering wheel positioned at an angle that doesn't allow you to sit with your arms in a neutral posture. Remember, the ideal posture for your arms is for them to be relaxed at your side with your elbows bent at between 90 - 110 degrees and your hands in the handshake position. If you adjust your steering wheel to an angle that allows you to drive in a posture close to this, the rate of muscular fatigue will be minimized. You also want to make sure though that the location of the steering wheel doesn't restrict your leg movement or vision of the dashboard instruments.
Remember, even if you implement all of the above tips you may still experience fatigue and discomfort if you don't pace yourself. This means stopping to take a break and walk around on a regular basis, every 1 - 2 hours. These breaks will permit your muscles to recover and should help prolong any discomfort or fatigue. Taking a break is also good from a cognitive perspective. Regular breaks help decrease your mental fatigue and improve your attention and focus on driving. Maybe we need more signs like the one below to remind us to take a break!
References and helpful web links:
http://www.drivingergonomics.com 2001 Loughborough University & HJ Consultancy
http://www.ctmonthly.net/archives/aug02/articles/feature1.html
http://www.ohcow.on.ca/english/handbooks/ergonomics_driving/Ergonomics_And_Driving.pdf
To Top
How to Prepare for an Ergonomics Assessment
There are a couple of tips that are helpful to be aware of before an ergonomist arrives at your location to complete an assessment. We thought it might be useful for you to know these as it makes both of our jobs easier and more efficient.
To Top
- If you are a unionized facility, make sure the Union is aware of what the purpose of the assessment is and what areas will be assessed. Depending on your agreements, it may be beneficial to have a union representative present during the assessment. Having a representative present has proven to be helpful, as they then understand first hand how the data is collected. Typically, this results in fewer questions and less controversy when the report is submitted.
- Identify a worker that can be observed, photographed and that has a complete working knowledge of the job to be assessed.
- Review injury or concern statistics on the job to be assessed. This will provide a historical perspective of potential concerns and can assist the ergonomist.
- Make sure you and the ergonomist understand how you intend to utilize the final report. Making sure both parties understand this is very important because it will allow the ergonomist to customize the report format to make it as usable as possible for you.
How to Apply Ergonomics Principles to Gardening Tasks
When we look at any job or task from an ergonomic perspective we consider the big three risk factors, Force, Posture and Repetition/ Duration. If you have attended any of our training sessions you will know that, typically, if you have two of the three risk factors present in a task there is a concern. Well, this is also true when we look at the job of gardening.
Usually, when it comes to gardening and yard work, we take advantage of good weather when we get it. As a result, this often leads to us doing these tasks on a repetitive basis or for a prolonged duration. If we get a day of good weather on the weekend we could garden or complete yard work for up to 8 hrs easily. Now, this in itself could be tiring but if we are working in awkward postures or with high forces we could be placing ourselves at risk.
In order to look at this easily, I have identified some key tasks and some tips that will help you work in a more ergonomically ideal manner.
Garden Tools and Equipment
Gloves
- Wearing gloves can help protect your hands when gardening but they can also make your job harder. If your gloves are too big, you will have to work harder to keep them on, as well as to grasp your tools. This means that if your gloves are too big, by the end of the day your muscles will be more tired, and may be more sore than if you were wearing a pair of properly fitting gloves
Hand Tools
- Before buying garden tools, it is important to think about who will be using them. If a number of different people, with different size hands, could be using the tools the handle size and style is very important. If there will be multiple users of your tools, it is recommended that the handle not have any grooves. This will allow each user to grasp the tool in a comfortable manner.
- It is also recommended that the tool handle be padded or rubberized to allow your grip to be comfortable.
- There are some "ergonomically designed" garden hand tools in the marketplace. You may find these beneficial if you have certain restrictions, or are gardening on a regular basis. However, remember just because you are using an "ergonomically designed" tool doesn't mean you are working in a better manner. You have to make sure you are using the tool correctly, with your hand and wrist in neutral postures.
Planting Pots
If you are planting pots, there are a couple of quick easy things that you should remember.
Your Posture
- Although the pots will typically be placed on the ground when they are planted, there is no reason they have to stay there when you are planting them. In order to minimize the amount of back flexion or stooping/squatting required, place your pots on your picnic table when you are planting them.
The Weight (or Force)
- When you are buying your pots, consider the weight of them. Sure a large ceramic pot may look nice but if you are unable to safely carry it is it really the best pot for you? Probably not.
- Okay, so now you have your pot on the table and are ready to start planting. If you fill the entire pot with soil, the pot will become significantly heavier. In order to keep the weight down, and aid in drainage, try placing some of your empty plastic pots in the bottom before adding the soil.
- Whenever you are moving the pots, remember to keep them as close to your body as possible and bend with your legs when you are lifting or lowering them.
Repetition
- In order to try and spread out the demanding tasks, it is recommended that you plant one pot and transfer it into location. Then, complete the next one. This way your back muscles will have time to recover between the lifting and carrying tasks.
Garden Work
Your Back Posture
- Planting in the garden can be hard on your back if you don't pay attention to your posture. If you are working on the edge of the garden, it is recommended that you kneel on the grass or on something soft. Arrange the plants to be planted and your tools around you so you don't have to reach or twist once you are kneeling down. Only plant the area directly in front of you, then stand up and move to your next location. Remember, twisting and reaching can be just as harmful as bending.
- If you are working in the middle of the garden, it can be hard to work in ideal postures. As a result, you need to remember to try to keep the curve in the lower part of your back when you bend forward (bend at the hips not the back). Since this can be hard to do properly, you should minimize the amount of time you spend in this posture and try to complete upright tasks in between to let your back muscles recover.
Yard Work
Once again, yard work is typically something we do all at once. If you have to do it all in one day, pay attention to these tips.
Repetition
- Try and break your tasks up into sections. Don't make piles of all of your yard waste, fill all of your bags, then carry them all to your storage area. Try to clean up as you go. When your pile is big enough, fill one bag and store it. This way your muscles are given a break and allowed to recover a little bit in between tasks.
Force
- If the loads you have are heavy, why not push them using a wheelbarrow instead of lifting and carrying them. It is recommended that if you have to carry a load more than 8.5m you should push or pull it instead.
Posture
- Another thing to pay attention to is your posture. Are you reaching and bending over when you are raking instead standing up straight and moving your body? Can you switch sides to share the loads with the other side of your body?
If you take your time and try to implement some of these tips you should be able to enjoy gardening without suffering discomfort the next day. Happy Gardening!
To Top
Options Inc. now accepts credit cards, specifically Master Card and VISA. We have added this payment option in response to requests from our customers. Hopefully you will find this payment option useful.
Please let us know if there are any other services that would be beneficial to you for us to offer. We are always open to learning about how we can better accommodate you.
To Top
We all know (or should know if you are on this website) what ergonomics is. But what is Participative Ergonomics?
Wilson and Haines (in Haines et al., 2002) stated that the participative approach is "the involvement of people in planning and controlling a significant amount of their own work activities with sufficient knowledge and power to influence both processes and outcomes to achieve desirable goals."
Participatory ergonomics is a 'multifactorial intervention'. That means the presence of the team has an affect on two risk factor levels. The ergonomic 'team' will make changes to the work place that reduces the physical risk factors present in a job. As well, participation in the process of change, including training, information exchange and decision making, all have the potential to influence psychosocial risk factors (Wells, 2002 and Haims and Carayon, 1998). Participation in the team increases the perception of job control and influence, increases feelings of importance and recognition and leads to improvement in self-confidence, competence and attachment of more importance to self determination (Mambrey et al, 1987).
Thus, participative ergonomics allows workers at different levels of an organization to be heard and to take part in changes to the work environment, tools, and processes that directly affect them. The result being that changes are implemented quicker, with fewer changes required and with employee buy in.
Some work places already use the participative approach in other areas of their work. These include quality circles, kaizen, continuous improvement committees and best ideas programs. The philosophy is similar. Employees know the job. They have knowledge that people who do not do the job every day do not have. This knowledge combined with the expertise of toolmakers, maintenance, engineers, etc. should result in the best solution for the problems.
In an application of participatory ergonomics in an office setting, Vink (1997), studied the effects of worker participation in the set up of their workstations. They found that the workers that took part in the set up showed the least deviation from the recommended workstation set up. This suggests participation had an effect on retention. In addition, the number of musculoskeletal complaints was reduced.
In a study of participatory ergonomics among hospital orderlies (Evanoff et al, 1999), researchers found that the formation of a Participatory Ergonomics team that implemented changes in training and work practices resulted in decreased risk of work injury, lost time, total loss days, compensation costs, and discomfort in the neck, lower back, forearms and knees. It also found improvements in job satisfaction, psychosocial stressors and social support.
It should be noted however, that a Participatory Ergonomics program will not work if the program is not implemented improperly. If a company is not ready or committed, if management views worker participation as a threat, if the Ergonomics Committee or Team is not provided with sufficient power, if workers feel their participation is not being considered in good faith, and if there is not full participation a negative outcome could result. In order to minimize these negatives aspects, a formal approach to using participatory methods needs to be developed.
How to set up a participative approach to ergonomics
Step 1: Obtain Upper Management Support
The decision to form a Participatory Ergonomics team needs to be made and supported by all Managers. One upper manager should be assigned as a "go to" person to prevent roadblocks. It is very important that this person supports the process and understands the need and purpose of ergonomics. Management, through policymaking, statements and public relations, needs to support and give power to the team. Management will need to decide how much decision making power the committee has. It has been shown that if little or no decision making power is given to the committee then success of the program is low. Finally, a specific funding source with adequate resources needs to be allocated to ensure recommendations are not stalled due to a lack of funding.
Step 2: Form Ergonomic Team/Committee
The main question here is who should be on the Committee?
Before this is determined, some decisions need to be made regarding the type of committee you are going to form. Is it permanent or will it be temporarily formed as problems surface? In large organizations, a permanent standing committee would be needed. However, in smaller companies a temporary sub committee, perhaps of the Health and Safety Committee, would be suitable.
The next decision to be made is the level of involvement of employees. Participation can be directed by the employee who has the concerns or by a representative for the workers in the area. In some cases, a team for each department may be required. In others, a representative from each department on one large committee is sufficient. It is best to include multiple disciplines or experts on the committee. Operators, supervisors, management, toolmakers, maintenance, engineering, plant nurse or doctor, etc. should be considered. In unionized work places representatives from both union and management must be present.
Once the committee or team is formed, the members will need to decide which issues to focus on. It is best to start with small projects and gain small positive results rather than have one large project fail.
Finally, is there an ergonomic specialist available and what is their role (training, team member, consultant, facilitator or guide of the process)? Some organizations choose to have outside consultants complete the assessment portion and make recommendations. The recommendations are then reviewed by the committee who decide if they are feasible.
Some additional questions that will need to be answered are:
- How will decisions be made?
- What level of influence is the committee given (impact on purchasing policies, corporate vs. plant wide)?
- What level of decision-making power does the committee have (makes recommendations to management, management decides to implement or committee makes decisions that stand)?
Step 3: Train all members
Once the committee is formed, all members and any persons who may be involved at the periphery should be trained. It is beneficial if all workers in a plant are provided with a basic form of ergonomic training to understand the need and purpose of the team. Team members should receive additional training on ergonomic basics, legislation, risk factors, identification, assessment, and design issues. Through the training, a framework for how the ergonomic process can work in the workplace should be made.
Step 4: Follow an Ergonomics process
A formal process and policy (see the attached as a rough example of an ergonomic policy in
Word or
- Identify and prioritize job risk
- Assess jobs
- Brainstorm solutions
- Implement solution
- Evaluate the Effectiveness of solutions
With a formal Ergonomics Team (using the participatory approach) in place, a smooth introduction of changes with resulting decreases in musculoskeletal risk should be achieved.
In all of our training courses we review a process for implementing ergonomics into the workplace. Details and content vary within each course. The decision of which course to take should be made depending on who is completing the assessment and solution/design stages within your team. Consulting on this, prior to training, is beneficial and will allow you to get the most useful information out of any course you attend.
Participative Ergonomics References and Resources
UW Participative Ergonomic Blueprint - http://www.iwh.on.ca/archive/pdfs/ergo_blue09_03.pdf
Carayon, P., Haims, M.C., Suh, H. (1998). Effectiveness of work organization interventions in office and computer work. Human Factors in organizational Design and Management - VI.291-298
Carayon, P., Smith, M. J. (2000). Work organization and ergonomics. Applied Ergonomics. 31, 649-662.
Evanoff, B.A., Bohr, P.C. and Wolf, L.D. (1999). Effects of a participatory ergonomics team among hospital orderlies. American Journal of Industrial Medicine, 35, 358-365.
Haims, M.C. and Carayon, P. (1998). Theory and practice for the implementation of 'in house' continuous improvement participatory ergonomic programs. Applied Ergonomics. 29(6), 461-472.
Haines, H., Wilson, J.R., Vink, P., and Koningsveld, E., (2002). Validating a framework for participatory ergonomics (the PEF). Ergonomics. 45(4), 309-327.
Mambrey, P., Oppermann, R., and Tepper, A. (1987). Experiences in Participative Systems Design. In: Docherty, P. et al. (eds.): System design for human development and productivity: participation and beyond. North Holland. Amsterdam et al., 345-358.
Vink, P and Krompier, MA (1997). Improving office work: a participatory ergonomic experiment in a naturalistic setting. Ergonomics. 40(4), 435-449.
To Top
Radiation Safety and Video Display Terminals (Computer Monitors)
When completing office assessments and office training we are often asked if radiation fields emitted by Video Display Terminals (VDT's) pose any problems. Those most concerned are pregnant women working long hours at the VDT.
From an investigation into this area we have found the following:
VDTs are essentially electrically identical to television sets. Both VDTs and television sets produce electromagnetic emissions (sometimes called radiation) from the CRT (Cathode ray tube); the phosphor (which is the chemical composition that coats the inside of the CRT screen); and from associated electronic components.
There are two types of radiation, ionizing and non-ionizing. Radiation that has enough energy to move atoms in a molecule around or cause them to vibrate, but not enough to change them chemically, is referred to as "non-ionizing radiation." Examples of this kind of radiation are sound waves, visible light, and microwaves. Also included in the non-ionizing electromagnetic radiation group are very low frequency and extremely low frequency electric and magnetic fields and electromagnetic fields (EMF).
Radiation that falls within the "ionizing radiation" range has enough energy to actually break chemical bonds. This is the type of radiation that people usually think of as "radiation". We take advantage of its properties to have x-rays taken, generate electric power, and in many manufacturing processes.
Both types radiation may be of concern to the VDT user.
The National Institute for Occupational Safety and Health (NIOSH), the U.S. Army Environmental Hygiene Agency, and others have measured radiation emitted by VDTs. The tests show that levels for all types of radiation are below those allowed in current standards. In fact, some measurements show radiation levels so low that they cannot be distinguished from general environmental radiation (background radiation).
OSHA has no standards that apply specifically to video display terminals or to extreme low frequency electric and magnetic field exposure. However, OSHA does have standards to protect employees against overexposures to radiation, noise, and electrical hazards.
In Canada, a Federal standard exists which requires all VDT distributors to control for X-ray emission such that no VDT can be sold in Canada unless the VDT meets or exceeds the standard (0.05 mR/hr). This standard is from any point on the external surface, which means whether someone is in front of, to the side of, or behind the display or receiver, they are protected against any potential emissions of the display to the same degree.
Reproductive Effects
Currently, OSHA has no reliable information that any birth defects have ever resulted from a pregnant woman working at a video display terminal. Furthermore, an article submitted from the Motherisk Program at the Hospital for Sick Children stated that epidemiologic studies and measurements of radiation do not suggest a reproductive hazard for video display terminals (Bentur and Koren, 1991). However, as the possible effects of radiation or extreme low frequency fields from VDTs on pregnancies continues to concern employees, NIOSH and others are currently conducting major studies to thoroughly investigate any potential problems.
The CSA guideline on Office Ergonomics states that although there is no conclusive evidence proving or disproving that EMF from VDT's constitute a health risk, low frequency emission detected very close to the surface of the VDT fall off very rapidly with any distance. As such, following basic office ergonomic guidelines as stated in our Design Guidelines and the CSA Guideline on Office Ergonomics will decrease potential exposures.
If you are interested in this area, the following references and links have more detailed information regarding the transmission of radiation from the VDT and reproductive risk.
References
The three most common occupational exposures reported by pregnant women: an update. Bentur Y, Koren G. Motherisk Program, Hospital for Sick Children, Toronto, Ontario, Canada Am J Obstet Gynecol. 1991 Aug;165(2):429-37
CSA-Z412, Guideline on Office Ergonomics, 2003.
Safety Code 6 published by Health Canada, Radiation Protection Bureau.
http://www.pc.ibm.com/ww/healthycomputing/vdt14.html
http://www.safetyoffice.uwaterloo.ca/hspm/documents/office_ergo/
electromag/electromagnetic.htmhttp://www.osha-slc.gov/pls/oshaweb/owadisp.show_document?p_table=FACT_SHEETS&p_id=170
http://hps.org/publicinformation/ate/cat64.html
To Top
Work Rest Schedules - A Means of Reducing Musculoskeletal Discomfort in Computer Work
Research into the area of work rest scheduling has been taking place for over three decades. With a rise in the use of computers by all levels of workers (data entry to executives) a relative increase in the number of musculoskeletal injuries has followed. Repeated trauma disorders were the dominant type of illness at 67% of all injuries (2000, Bureau of Labour Statistics). Not only are musculoskeletal injuries of concern, but visual fatigue and job stress are affected as well.
Employers looking for a means of reducing musculoskeletal injuries, visual fatigue and job stress in the workplace may first look to change the work environment, but often find they are unable to control all of the factors. They may then look at changing workers postures. However, controlling the workers postures or implementing fully adjustable workstations to ensure all workers can work in optimal task specific postures can be difficult or not affordable. As a result, the employer then looks for an alternate means of reducing injuries. One such method is the implementation of a work rest schedule. Work rest scheduling has often been used in industry to reduce the risk of injury for workers exposed to high manual material handling risks and risks due to working in high or low temperature extremes.
Work rest scheduling, in conjunction with changes to the workers posture, is an ideal method to reduce computer related risks. However, implementing a work rest schedule to a work place can be a daunting task that raises many questions.
- What length of break is necessary to encourage muscle recovery and eyestrain reduction?
- Will productivity decrease if my employees are taking frequent breaks?
- What effect will the break have on my work i.e. being interrupted by these breaks?
- How will I know when I should take a break?
Recent research in this area has shown that computer users that take more frequent rest breaks benefit from not only a decrease in musculoskeletal discomfort but also an increase in productivity (NIOSH, Sauter and Swanson, 1992, Swanson and Sauter, 1994). However, it has also been shown that even when employers encourage workers to take rest breaks, they may not take them or they wait until they feel discomfort in a body part before taking them, which is too late.
How frequent and how long should rest breaks be?
Breaks need to be taken before any discomfort occurs. If you take a break when you begin to feel discomfort, it will take longer for your muscles to recover than if you take a break earlier. Breaks need to be long enough, and frequent enough to allow for muscle recovery to occur. Spontaneous breaks of only five to 10 seconds are not sufficient to allow for muscle recovery. In addition, muscle recovery needs to be ongoing throughout the workday in order to maintain low muscular stress levels. If short, more frequent rest breaks are taken; problems and any body discomfort can be prevented entirely (Henning, 1997).
Various studies have examined the length and frequency of rest breaks.
- Boucsein and Thum (1995) suggest a 7.5 minute break after 50 minutes of VDT work until noon and 15 minutes after 100 minutes of work in the afternoon.
- NIOSH has recommended a 15 minute break for every two hours of moderately demanding VDT work (or for every one hour of intensive VDT use). The NIOSH study also suggests that the schedule of a 3 minute break every 50 minutes with 30 second breaks every 10 minutes is also effective.
- Henning et al (1997) - Examined the effects of a three minute break every 60 minutes with 30 second breaks every 15 minutes
- Balci and Aghazadeh (2003) examined three different work rest schedules, one 10 minute break after 60 minutes of work, one five minute break after thirty minutes of work and micro pauses consisting of 3-30 second and one 3 minute break as stated above.
So, which frequency and length of break is best?
To decide this lets look at the reduction in the discomfort ratings and any productivity changes that occurred in each of these studies.
- Floru et al, (1985) found that a 5 minute break after 40 minutes of work eliminated the performance decrements that would normally occur in work without breaks.
- Henning et al (1997) found that well-being and productivity increased in one work place and did not change in another work place when rest breaks were introduced.
- Balci and Aghazadeh (2003) found that a work rest schedule consisting of 3 - 30 second breaks and 1- 3 minute break, broken up over one hour (in addition to regularly scheduled breaks) resulted in lower discomfort in the upper extremity and improved speed, accuracy and performance in both data entry and mental requirement tasks completed in a lab setting.
- A recent NIOSH study tested a schedule of 3 minute breaks every 50 minutes, with 30 second micro pauses every 10 minutes. The results of the study showed a decrease in worker discomfort and a significant increase in productivity compared to the traditional schedule of midmorning and mid afternoon breaks. Two insurance companies that instituted this schedule found the efficiency of claims processing was higher during the test period than in a typical earlier period. (http://www.kalpoint.com/kalpoint/education/code/ver4.2/righton.htm)
What constitutes a rest break?
Rest breaks are defined as periods of time when the worker is doing something other than working at the computer. This could be working at their desk, handwriting, faxing, photocopying, filing, etc. Work breaks during which workers completed stretches were found to have an increased lowering affect on eye and leg discomfort (Henning, 1997).
We have shown thus far that rest breaks can have a positive affect on muscular and visual discomfort and that productivity is either not affected or is improved. How can rest breaks be implemented such that the worker does not feel interrupted and will take these needed rest breaks? Some of the reasons for low compliance to taking rest breaks are,
Repetition
- Work is interrupted,
- Pay is based on performance and the worker feels they will lose pay if they take additional breaks, and
- Psychosocial influences within the office.
Henning (1997) found that lack of compliance in taking these breaks was due to the inability to integrate rest breaks into the type of tasks that were being completed.
In order to choose an appropriate and effective work rest schedule, you need to take into consideration the work tasks. Are the workers completing data entry, composition, telephone and computer work simultaneously, client based or client driven work? Do the workers have deadlines, incentive pay or quotas to meet? Once the type and pace of work is identified, an effective method of merging rest breaks in or around the tasks must be completed. The best work rest schedule is one that workers use and does not significantly interrupt their work duties.
Here are some methods of indicating when rest breaks should occur:
Automated - The workers computer or lights indicate when a break is required. The time is usually predetermined and does not take into consideration what the worker is doing at the moment or if a break is possible (i.e. worker is on the telephone with a client, looking up information). An example of this type of break would be stretching software where the software is programmed to break at a set interval. During that break, the program gives instruction on stretching. This program provides the workers with a break but does not take into consideration the tasks and can be bypassed by the worker.
Self-regulating - This relies on the worker to take breaks at appropriate intervals. Although the workers would be educated on the need and benefit of short, frequent rest breaks this method leaves it up to the worker to initiate the break. Thus there is no guarantee of compliance or indicator to the worker when a rest break is required.
Self-regulating with feed back - The worker is required to take their own breaks but feedback, such as total continuous time at the computer, is provided via a small icon on the computer monitor. This method allows the worker to monitor their total computer time and adjust their breaks around the tasks that they are required to complete.
There appears to be sufficient evidence to suggest that an increase in short rest breaks is beneficial for computer workers. The decision to implement a work rest schedule and how it will be conveyed to the workers should be undertaken with consideration of workers tasks, worker preferences and an assurance that all workers are educated on the need for these breaks.
As a final note, although work rest scheduling is a means of providing recovery to muscles in hopes of reducing musculoskeletal injuries it should not, on its own, replace education on proper working posture and proper design of a workstation. When possible, changes should be made to ensure the worker is working in an optimal position for the task.
To Top
Ergonomics: Manual Materials Handling
As presented in Government Purchasing Guide November/December 2003 Vol. 35, No.6
By Kirsti MacAulayInjuries caused by manual materials handling (MMH) used to be thought of as primarily related to people in shipping or other jobs traditionally involving manual labour. However, it has become apparent that these types of injuries can-and do-affect workers in different kinds of work environments, including offices and hospitals. Workers in these environments are all handling different things, from parts to people, but the same principles apply to all of them.
In Canada, for the year 1998 (1):
- overexertion accounted for nearly 25% of all types of occupational injuries;
- sprains/strains accounted for 40% of all time-loss injuries;
- back problems were the most common type of time loss injuries;
- the three most common sources of occupational injuries were bodily motion, working surfaces, boxes, barrels, containers and packages; &
- the total number of time-loss injuries from sprains/strains had decreased since 1994.
Manual material handling risks
When looking at MMH risks, one must consider the physical demands of a given job or task. This requires evaluation of the job's physical ergonomics, including the main risk factors-posture, force and repetition.
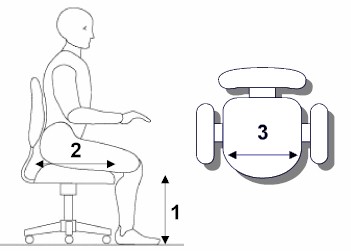
The posture risk comes from working in awkward or non-neutral body positions. Awkward postures require a worker to bend or twist his/her joints beyond neutral zones. The ideal neutral posture is shown in Figure 1. To calculate risk, the postures the human body moves through to complete a task are all assessed and compared to this diagram. It is important to consider the entire body, from head to toe.
Figure 1
The force risk relates to the amount of work (e.g. lift/lower, push/pull and carry) a person must perform in excess of his/her safe strength limits. What are the weight and dimensions of the load? Is it a stable load? Does it involve handles? These are all relevant questions in establishing the safe strength limits for the worker.
The repetition risk exists when a worker is required to perform the same movement or sequence of movements many times during a given period, as there is not enough opportunity for muscle recovery to occur. How many times is a given task completed within a shift-or within one hour? At what frequency of action is the person required to work? These are relevant questions that help quantify the demands placed on the worker.
Types of injuries
Depending on what risk factors are present, the types of injuries a worker is susceptible to will vary.
If a worker is exposed to a job whose demands minimally exceed his/her physical strength capabilities on a repetitive basis-or is required to work in awkward postures on a repetitive basis-he/she could develop a repetitive strain injury (RSI). This type of injury develops on a gradual basis. Sometimes, it can do damage before the afflicted worker even realizes it.
The second major type of occupational injury is acute trauma. This is caused when an exerted force exceeds the tolerance of the associated soft tissue-such as muscle, tendon or ligament. This can result from trying to exert more strength than you are capable of-for example, trying to lift an item that is too heavy for your strength capabilities.
Posture
Each joint has an ideal posture associated with it. This is typically within a range of motion closely surrounding the neutral posture of the joint. As a result, you need to assess a given task to determine if you can complete it while maintaining an ideal posture at each joint.
As an example, you should keep your back in an ideal posture when completing all types of MMH. Specifically, you want to keep three curves present in your spine (Figure 1), regardless of how much you have to bend or how far you have to reach. Maintaining the three curves will mean the strongest and most stable posture for your spine.
Force
How do you know what an acceptable weight limit is? The answer is not easy, as a lot of variables come into play.
As a starting point, it is worth knowing in a "perfect situation"-which almost never exists-the maximum recommended weight limit is 23 kg (51 lbs) (2). The recommended weight limit decreases significantly if any/or all of the following occur:
- the load cannot be held close to the worker's body;
- the load is not equally balanced;
- the load does not have handles;
- the load is not handled in a symmetrical manner; &
- other parameters are less than ideal.
Repetition
A job or task becomes repetitive if the job cycle is less than 30 seconds or if more than 50 per cent of the cycle time is spent performing the same fundamental cycle (3). "Cycle time" is the amount of time it takes to complete all essential tasks of a job. If a task is repetitive, sometimes the risk can be contained-on an interim basis-by implementing work pacing strategies or job rotation.
Work pacing strategies include dividing up MMH tasks throughout the shift. The worker's musculature is thus able to recover between tasks, minimizing the loss of strength and stability due to fatigue.
If a task cannot be split up over a shift, job rotation can be considered, as an alternate, short-term containment method. By rotating the worker out of the job, the repetition rate and fatigue factor will be minimized and the risk will hopefully be contained.
Hospitals and nursing homes
When handling patients in hospitals and nursing homes, the shape, size or weight of the loads cannot be changed. As a result, when MMH demands exceed safe limits for workers, alternative methods of patient handling must be investigated.
The ergonomic risks associated with patient handling have received significant attention over the past year. The Occupational Safety and Health Association (OSHA) has developed Guidelines for Nursing Homes: Ergonomics for the Prevention of Musculoskeletal Disorders (4). This document recommends manual lifting of residents be minimized in all cases and eliminated when feasible.
For this purpose, an analysis should be carried out of any resident lifting and repositioning tasks. This analysis must incorporate the needs and abilities of the residents involved.
From an equipment and policy perspective, manual handling demands can be decreased by:
- increasing the use and availability of mechanical lifts;
- increasing the use of no-friction pads/sheets during transfers and repositioning tasks; &
- ensuring workers function in pairs when supporting or transferring patients.
Offices
The office is not typically thought of as an environment with many inherent MMH concerns. As a result, the concerns that do exist are not commonly addressed or acknowledged.
Some common concerns are related to boxes. Stacks of photocopier or printer paper can be heavy and-depending on how the boxes are stored and whether or not handles are used to lift and carry them-can exceed the strength capabilities of workers.
Another common concern is with "banker's boxes," which are used for storing paper documents. If these boxes are filled to capacity, they can exceed the "perfect lift" limit of 23 kg.
In addition, if workers are placing the boxes on high shelves, not using the handles, carrying them instead of placing them on carts or handling them on a repetitive basis, the recommended weight limit becomes lower-and the level of concern increases. To address this problem, the standard banker's boxes could be filled only to half capacity or smaller boxes could be purchased instead.
Points to remember and consider
It is crucial to educate workers about the importance of:
- completing all MMH tasks with caution;
- following good MMH principles; &
- using available tools and handling equipment.
Applying such principles should result in a safer, happier and more productive workforce.
Kirsti MacAulay, CCPE. Kirsti is the Principal Ergonomist at Options Inc., a professional ergonomic consulting firm that has been servicing Ontario since 1999. For more information on Options Inc. visit www.oiweb.com, or to contact Kirsti, email her at kmacaulay@oiweb.com
Notes
(1) Occupational Injuries and Their Cost in Canada 1993-1997, Research and Analysis Section, Occupational Safety & Health and Fire Prevention Division, Labour Branch, Human Resources Development Canada.
(2) NIOSH Revised Lifting Equation, National Institute for Occupational Safety and Health, 1994.
(3) Silverstein T, Fine L, Armstrong T. Occupational factors and carpal tunnel syndrome. Am J Ind Med 11:343-358, 1987
(4) Additional information about this document can be found on the OSHA website at www.osha.gov
To Top
Prevention of Work Related Upper Extremity Musculoskeletal Disorders
By Jennifer Enns, Associate Ergonomist CCPE, MSc. Candidate, University of Waterloo
Work-related musculoskeletal disorders (WMSD) of the upper extremity are a major cause of worker impairment, disability and compensation in many hand-intensive occupations. These disorders represent significant burden to companies and those concerned with health care and workers compensation schemes. WMSD's have complex multifactorial etiology including physical aspects of an activity like force, adverse postures, repetition, duration, and vibration as well as psychosocial factors (Hagberg et al, 1995). The prevention of WMSD is a major priority.
Prevention of WMSD deals with three main aspects: primary, secondary and tertiary prevention.
- Primary prevention is the prevention of the first indications of illness or injury. This is completed through task analysis and ergonomics interventions.
- Secondary prevention involves reducing the risk of disability, or enhancing the ability of those with symptoms. This is completed through rehabilitation and the prevention of the development of impairment.
- Tertiary prevention involves enhancing the return to work or the other productive and healthful activity, and preventing recurrence.
A variety of assessment models exist for determining exposure risk for the upper extremity WMSD's. Good ergonomic tools record and rate risk factors, as well as, rate the injury risk to the upper limbs or the intervention priority (Wells, 1999). Tools are either designed for screening purposes or for more definitive analysis. Some of these models include RULA, Strain Index, ACGIH-TLV (Threshold limit value), EMG analysis of muscular activity (APDF, gap analysis, and EVA), force matching, and various checklists. Keep in mind that each method has strengths and weaknesses.
It is well accepted that the occurrence of WMSD's can be reduced by ergonomic interventions. These interventions can be classified as engineering controls (i.e. workstation and tool design, work reorganization and station labour, work/rest cycle, job rotation), administrative controls (i.e. participatory ergonomics programs), and modifier techniques (i.e. worker training and education, exercise/stretching programs and physiotherapy).
A common method of secondary and tertiary prevention of WMSD's of the upper extremity is the use of braces and splints, including forearm support bands for lateral elbow pain. Although it is widely accepted that forearm support bands reduce forces at the tendinous insertion of the wrist extensors, the effect is not well understood. Many theories on the mechanism of these bands exist and further research is required to clarify these theories and the efficacy of forearm support bands.
A summary of some intervention studies is provided below. Collectively these studies indicate positive evidence for implementation of ergonomic interventions. For a more comprehensive review of additional studies as well as guidelines for intervention studies, refer to reviews by Westgaard and Winkel (1997) and NRC (2001).
Author: Aaras et al., 1998 Work Areas: Technical division, software delivery, & office workers Intervention: New lighting, workplaces, & optometric intervention Study Design: 2 year prospective epidemiological field study; two intervention groups & control group Measures: Questionnaires dealing with headache, visual conditions & discomfort, Musculoskeletal pain, organizational & psychosocial factors; VAS; postural load via EMG of trapezius & joint angles Results:
- Reduction in visual discomfort & shoulder & neck pain,
- Lower trapezius EMG with forearms rested on table in redesign,
- Decreased static load,
- No change in forearm/hand pain
Comments: The lack of a significant difference in forearm & hand pain may be due the time the operator used the mouse. Author: Galinsky et al., 2000 Work Areas: Data-entry operators Intervention: Supplementary rest schedule with two additional 5 min. breaks in morning & afternoon Study Design: Field study; 42 participants Measures: Feeling state questionnaires (4 times daily; ratings of body discomfort, visual blurring & mood) & rest break questionnaire (report number & duration of actual breaks) Results:
- Discomfort of several body parts was reduced,
- Day-to-day increases in discomfort in forearm, wrist & hand during the workweeks decreased,
- No effect on productivity
Comments: Rest breaks provided opportunity to recover from fatigue imposed by static postures & repetitive motions Author: Hakkanen et al., 1997 Work Areas: Trailer assembly workers (furniture assembly & fixing) Intervention: Implemented jigs; more effective tools with suitable handle shape & higher friction; hoist; new placement of storage of parts; adjustable table; work enlargement. Study Design: Longitudinal study; 19 month follow-up; 33 participants Measures: Video analysis; Upper extremity exposure during driving screws & drilling was computed based on experiments on force & time requirements Results:
- Number of repetitions
- Less deviated wrist,
- Cumulative exposure on UE was lower in furniture fixing tasks,
- Lifting with twisting torso
Comments: Relatively simple and low-cost solutions decreased exposure of risk factors of WUEMSD Author: Mirka et al., 2002 Work Areas: Furniture Manufacturing Intervention: New & modified hand tools: new upholstery hand tool that used power grip instead of pinch; sander securing hand; spray gun Study Design: Experimental laboratory evaluation of interventions Measures: Goniometer; EMG of Finger flexors and extensors, generalized thenar group, FDI Results:
- New sander interface reduced extensor muscles,
- Upholstery hand tool reduced intrinsic hand muscle activities,
- Spray gun reduced wrist flexion & ulnar deviation
Comments: Recommend follow-up with an epidemiological study on injury stats Author: Westgaard & Aaras, 1985 Work Areas: Small manufacturing plant; (cable making & 8B system) Intervention: Adjustable mounting system; Improved illumination; adjustable arm rests; lighter gun with counterbalance Study Design: Longitudinal epidemiological with 8 year follow-up Measures: Interviews concerning feelings of discomfort & pain while working; EMG of upper & lower trapezius Results:
- Decrease in m-s sick leave,
- Labour turnover,
- Severity of symptoms,
- Mean muscular load,
- Improved productivity
Comments: Ergonomic interventions had a clear positive effect; recommend further changes to further decrease static muscle load References
Aaras, A., Horgen, G., Bjorset, H., Ro, O., & Thoresen, M. (1998). Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. Applied Ergonomics, 29(5), 335-354.
Armstrong, T. J., & Lifshitz, Y. (?). Evaluation of jobs for control of cumulative trauma disorders
Chaffin, D. B., & Andersson, G. B. J. (1991). Occupational Biomechanics. Second Edition. John Wiley & Son, Inc. New York.
Galinsky., T. L., Swanson, N. G., Sauter, S. L., Hurrell, J. J., & Schleifer, L. M. (2000). A field study of supplementary rest breaks for data-entry operators. Ergonomics, 43(5), 622-638.
Hakkanen, M., Viitari_Juntura, E., & Takala, E. (1997). Effects of changes in work methods on musculoskeletal load. An intervention study in the trailer assembly. Applied Ergonomics, 28(2), 99-108.
Lintula, M., Nevala-Puranen, N., & Louhevaara, V. (2001). Effects of Ergorest arm supports on muscle strain and wrist positions during the use of the mouse and keyboard in work with visual display units: A work site intervention. International journal of occupational safety and ergonomics, 7(1), 103-116.
Mirka, G. A., Shivers, C., Smith, C., & Taylor, J. (2002). Ergonomic interventions for the furniture manufacturing industry. Part II - Handtools. International Journal of Industrial Ergonomics, 29, 275-287.
National Research Council and the Institute of Medicine (2001). Musculoskeletal disorders and the workplace: Low back and upper extremities. Panel of Musculoskeletal Disorders and the Workplace. Commission on Behavioural and Social Sciences and Education. Washington, DC: National Academy Press.
Silverstein, B. A., Fine, L. J., & Armstrong, T. J. (?) Carpal tunnel syndrome: Causes and a prevention strategy
Wells, R. P. (1999). Integrated analysis of upper extremity disorders. In: Occupational Ergonomic Handbook. Karwowski, W. & Marras, W. S. (Editors) New York: CRC Press.
Westgaard, R. H., & Aaras, A. (1984). Postural muscle strain as a causal factor in the development of musculo-skeletal illness. Applied Ergonomics, 15(3), 162-174.
Westgaard, R. H., & Aaras, A. (1985). The effect of improved workplace design on the development of work-related musculo-skeletal illness. Applied Ergonomics, 16(2), 91-97.
Westgaard, R. H., & Winkel, J. (1997). Ergonomic intervention research for improved musculoskeletal health: A critical review. International Journal of Industrial Ergonomics, 20, 463-500.
To Top
Children, Computers and Ergonomics - Can they fit together?
As the use of computers and the internet in our world becomes a necessity, the number of computers in the home rises each year, as does the number of children using computers on a daily basis, the amount of time they spend on the computer and the number of computers in the classroom. It is estimated that children use computers in the home and school between 1 - 3 hours per day with computer use highest among 8 - 12 year olds (72%). In the US, 98% of schools (K - 12) have computers or 4.4 million computers are in the classroom. In Canada, nearly 9 in 10 young Canadians have a computer at home, with the majority having access to the Internet, according to StatsCan. With the increasing time children spend on computers you would think that computer ergonomics, which is applied often in the adult computer world, would be applied to the child at home and in the classroom. This however, that is not the case.
There is some evidence that suggests that children are becoming afflicted with the same computer-related repetitive strain injuries as adults. A 2002 British study of 1,000 schoolchildren found that 36 percent of 11 to 14 year olds, suffer serious, ongoing back pain related to their use of computers. (Peter Buckle, of the Robens Centre for Health Ergonomics at the University of Surrey in England). Interestingly this number may be low as another study (Royster and Yearout, 1999) found that children are less likely to report discomfort they experience while using a computer and more likely to continue with the discomfort than children that are playing sports or a musical instrument. With an underreporting of discomfort, accurate measures of the prevalence of this problem are difficult to obtain. Further, children are also less likely to make changes to their computer set up and ignore problems that would be addressed by adults. This makes it extremely important to not only educate our children on proper workstation set up but to educate parents and teachers so that issues can be pointed out and corrected early.
There are, however, people who disagree with this stating that children are not using computers for lengthy time within the school atmosphere and therefore they are not at risk for developing injuries (Williams et al, 2000). Even if this is the case, children are spending increasingly more time on the computer at home. This increased time at home, plus computer work at school, combined with improper postures due to equipment not made for children, can expose them to risk factors and increase their risk of developing computer related musculoskeletal disorders. Further, even if the overall risk for the development of musculoskeletal disorder is proven to be low, the habits children learn now will follow them into adulthood (Shinn et al, 2002). Hence teaching children good posture when working on the computer could be invaluable to their future working lives.
Where do the problems lie with children and computers?
If we examine the issue from a risk factor point of view, the use of computers by anyone has the potential expose the person to two primary ergonomic risk factors: 1) Posture; 2) Repetition and 3) Duration. It should be noted that the risks to children whose bones and muscles are still developing might be increased.
Posture
The postures assumed when working on a computer are reliant on the equipment that is available to the user. Adjustable equipment is ideal but most workstations can be made appropriate with a few minor changes. Most computers workstations within schools consist of a standard desk and stacking type chair both of which have little or no adjustability. In a 1999 study (Oates et al in Straker, 2000) investigating the posture of children in school, they found that no workstation was adjustable, all exceeded recommended dimensions and that all student postures were in the unacceptable range. Lets examine the concerns with each aspect of the workstation separately.
Desk
- Students use monitors that are too high resulting in extended neck postures
Keyboard and mouse
- The keyboard and mouse are often positioned on the desk. This is too high resulting in abducted shoulders, flexed elbows and wrists.
Chair
- When seated children sit either too far forward and end up perching at the end of the seat, or too far back and end up slouching in the chair.
- They either do not, or cannot, use the back support in the chair. Often these types of chairs have little or no low back support.
- When seated in the chair, the children's feet dangled off the ground and the back of the chair pressed on the back of their legs.
Laptops
- Laptops by their design introduce posture issues. Since the screen and keyboard are connected it is difficult to get both into an optimum position. Either the arms and hands or the neck are placed into an awkward posture.
- The weight of a laptop can vary and this weight may introduce problems when it must be carried from place to place.
Repetition and Duration
At a computer workstation both repetition and duration are important issues to consider. Repetition is an issue with respect to keying and mousing movements of the fingers and wrist, and duration is an issue for the back, neck, shoulders, legs and feet due to the length of time spent in a seated posture.
Lighting
Lighting, vision and posture are all interrelated. It is known that we change our posture to avoid certain visual problems, such as glare or not enough light. These visual problems can then lead to concerns in the head, neck, and shoulders. Lighting issues in the classroom are usually related to too much light being present for computer use. Further if the computer screens are oriented incorrectly, glare will result from either the overhead lights or the windows. Improper lighting can also have an affect on vision. Eyestrain, headaches, blurred distant or near vision, dry or red eyes, double vision and light sensitivity can all occur if poor lighting is present. This is often referred to a Computer Vision Syndrome and although it is often seen in adults it is increasingly being seen in children.
Now that we know the issues, what can you do to help out?
Limit the time at the computer
Setting limits on the time that a child spends on computer is needed for many reasons, one of which is to reduce the chance of injury. Studies have shown that children that use the Internet more than 3 times per week spend only 2/3 the amount of time reading as children who do not use the Internet. These children also scored lower on tests of spelling grammar and punctuation. Additionally, with the number of overweight and obese children rising, limiting the time at the computer could be important to encourage physical activity. Further, being healthy and active has been shown to decrease risk of injury in adults and may have a similar protective affect in children.
Breaks
Encourage taking breaks away from the computer both for body movement and for the eyes. This could be stretching, walking around, or looking out the window (eyes). In schools, breaks should be incorporated in the lessons ensuring that children are not working at the computer for more than 45 - 60 min. without having a break for a change of position. Encouraging children to look away from the computer every 20 min. will have a beneficial impact on vision problems due to the computer. There are also computer programs available the can be placed on the computer, notifying the user when it is time to take a break.
Look for appropriate equipment for children
A search of the Internet for equipment designed for children to use at computers did not turn up many products. What is available tends to be "kid themed" but does not have much adjustability. Some products only offer height adjustment. In fact, an examination of the height adjustment ranges showed only a 0.5 to 2.25 inch difference from the average adult adjustable chair. Chairs for children need to either adjust lower to allow them to work at a lower surface height, or be raised higher to bring the smaller children up to the adult sized desk. A footrest would then be needed.
The limited products available include child-sized desks, mousing devices and keyboards. These are made smaller, and fit the body and hands of children better. The keyboard keys are larger and brightly coloured with the overall size of the keyboard being smaller than your typical keyboard. Sometimes children like to use trackballs instead of mouses because they find them easier to handle with their small hands. A small mouse would be just as effective. Remember, keep the mouse and keyboard at the same height and try to keep the mousing arm close to the body.
There are many desks that are available and marketed as specifically for children. However, of those viewed, few were found to meet the needs of children using a computer. If you are buying a desk for you child, have them try it out, see if it allows them to use neutral postures, and has some adjustment. When making a big purchase like this you also want to make sure that the piece of equipment can grow with your child. Remember, if you are buying a workstation for use by the entire family, adjustability will be the most important factor to consider. www.askergoworks.com is a website that has some kid friendly equipment, available for different age groups, designed with ergonomics in mind.
Changes to current equipment
By adding small pieces of equipment (from a store or around your house) your current workstation can be made more ergonomically correct. For examples, view the pictures below. The first picture shows a child working at a computer, a normal sight in most households. The second picture shows the same desk with some modifications i.e. using a box as a footstool, a different chair and a pillow for added back support. Although the height of the monitor is not ideal, the typing and sitting postures are much improved. Further, in the third picture an older child is now using the station and only slight changes were required. This set up is excellent for either child.
To make changes to a workstation you can use stools or a box as a footrest, place a cushion on a chair to raise the seated surface and/or provide more back support, or sit on books or use books to increase the height of the monitor. If you were thinking about purchasing one piece of equipment to try to improve the computer workstation for all users, we would recommend the purchase of a height adjustable keyboard tray. An adjustable keyboard tray is beneficial for both adults and children. It will allow any user to improve their shoulder, elbow, and wrist postures. Then, if required, further changes to the chair and monitor height could be made as stated above.
Laptop solutions
To set up a laptop effectively, use an external keyboard and mouse and then mount the laptop on a monitor riser (if needed). In order to store and transport the laptop safely and effectively, ensure you have a well-padded, comfortable carrying case for it.
Lighting
The desk should be set up perpendicular to the windows and any lighting. This way, the computer monitor will be parallel to both, thus minimizing the chance of glare occurring. If there is a concern, the amount of light in the room should be measured and compared to standards (40-50 footcandles, recommended for computer areas, Anshel). If required, removing bulbs or turning some lights off could help address lighting and glare concerns.
Education
Take time to learn about the proper set up for computer workstations yourself so that you can teach your children about ergonomics and how to sit at a computer. It is important to monitor their computer use, comment on their posture and make changes as stated above if necessary.
If possible, you should also take a look at your child's workstation set up at school and investigate whether or not you can make minor changes to improve it. There are computer programs on the market geared at teaching children and their parents about ergonomics. Further, local ergonomic companies would probably welcome an opportunity to come into the classroom to give a presentation on ergonomics and repetitive strain injuries to students.
For detailed information on how to set up a computer workstation, refer to the Office Ergo Online tool. This is a free tool that steps you through how to set up your workstation and provides information on repetitive strain injuries. This tool is set up for adults but all recommendations are made to improve posture and therefore can be applied to both adults and children. The additional recommendations included within this paper should also then be applied to ensure children are set up at their computers correctly. Some other good resources are www.ergonomics4children.org and www.ergonomics4schools.com.
Budget-minded Solutions/Ergonomic Tips for schools
Many schools have probably not included ergonomics as part of their programs due to the costs often associated with the implementation of such programs. However, there are some minor changes that may be possible that have minimal or no costs associated with them.
- Determine if the current equipment can be adjusted at all;
- Survey classes to get an idea of the height ranges of the users;
- Make adjustments to the equipment as needed - providing several heights of desks or sizes of chairs in each classroom may be warranted;
- To keep costs down, investigate if the parents association can be involved in making adjustments to equipment;
- If you do have adjustable equipment, ensure all students and teachers understand the need for and how to adjust it;
- Obtain or make footrests - investigate if your school or a local high school can make footrests as part of their woodworking program;
- Where no changes can be made to the workstation, ensure that all students are educated on taking appropriate breaks and are given stretches. Full training on proper computer posture may not be required if they will not be able to apply the principles. Stretching programs can be downloaded from many reputable websites for no charge or you could have a co-op student complete this as part of a project;
- If you don't have a mouse tray, at least make sure that the mouse is close to the side of your body. This is necessary to ensure that your upper arm can remain relaxed and your posture can remain as neutral as possible;
- Wrist rests should generally not be used as actual resting places for your wrists. This is because wrist rests, especially the very soft, cushioned kind, actually contour to the wrists and encourage wrist-twisting movements;
- Never use the "legs" that many keyboards have attached on the bottom surface of the keyboard. Using these legs would place the keyboard at a positive slope (slant the keyboard towards the operator), which should be avoided.
The ideal computer workstation posture
Recommendations for Purchasing Computer Chairs for Children
Recommendations for a suitable chair for children when at a computer do not differ in the requirements but do differ in size, from adult recommendations. The following is an outline of recommendations using children's anthropometric data (DTI, Pheasant, 1988). This document could be used as a guideline for the purchase of chairs by the individual or by an institution (i.e. school).
A chair should be easy to adjust from the seated position, adjustment controls should be clearly marked, and no special training should be required to use the chair. The chair should have a waterfall front edge of seat with foam cushioning in the seat and backrest.
Seat height (1)
- Optimum height for use when sitting in the upright position is the popliteal height plus the thickness of footwear.
- Seat height should be readily adjustable by the user.
- Seat height should accommodate the smallest to the largest child. This will vary with the age of the children.
- Popliteal height varies from 26 cm for the 6-year-old smallest child to 43 cm for the tallest 12 year to 48.5 cm for the tallest 18 year old. Based on this, the seat height of a chair should range from 26 cm to 48.5 cm to allow all users to touch the floor flat footed. Alternately, chairs can be chosen based on the age of the population using it. This would make the range of height adjustability required smaller.
- When considering seat height for children you must also take into consideration the type of desk. If the child were using a smaller desk, then a chair that can be lowered so that the child could touch the ground flat footed would be recommended. However, if they were using a regular adult sized desk then a chair with higher height adjustment would be required to increase the child's seated height. As a result, a footrest would then be required as the child would no longer be able to touch the ground with their feet flat. An empty box, stacked books or footstool could all be used as a footrest.
Seat Depth (2)
- Optimum seat depth for use when sitting in the upright position is slightly shorter than the anthropometric measurement of buttock to popliteal length.
- Legs should be positioned without compression from the chair on the back of the knee.
- Seat depth adjustment is desirable to accommodate the smallest to largest child. For children ages 6, 12 and 18 the seat pan depth should be 27, 49 and 55 cm respectively, to ensure all children at each age could sit comfortably.
- If one chair is required to accommodate ages 6 through 18, the chair should have a seat pan depth of no more than 27 cm. Alternately several sizes of chairs, with varying seat pan depths could be made available.
Seat Width (3)
- Important to allow room to get in and out of the chair and to reposition or change postures as required.
- Provide room for clothing and armrests.
- The minimum dimension for the seat width should accommodate the distance across the hips 18, 35.5, 39 cm for 6, 12 and 18 year old children respectively.
Back Support
- Need to examine backrest height, lumbar support, backrest width, and backrest angle.
- Backrest height and width should provide adequate support to the back
- Backrest angle should allow backward movement from 90 to 110°.
- Lumbar support - convex vertically and concave horizontally to fit the low back curve.
Arm rests
- Provide support to the muscles of the neck and shoulders. It should be noted that armrests are not required and may not be beneficial for all workers. Users of smaller stature and width may find the armrests too far apart. As a result, adjustable width armrests may become an important component of a chair.
- Should not restrict the workers preferred posture or access to the workspace, and should be comfortably padded to reduce contact stress with the forearms.
Footrests
- Are necessary when the height of the chair does not allow the person to rest their feet flat on the floor.
- Should be used when the work surface height is fixed and the person adjusts their chair to keep arms and shoulders comfortable, thus raising their feet off the ground.
- Allow changes of leg postures, most comfortable at 90° ankle angle.
- Should not move unintentionally while in use.
Casters
- Are recommended for work chairs at computer stations.
- Should suit the floor surface.
- Should not travel unintentionally when occupied or not occupied.
- A five point, or five caster, base is the most stable and will prevent tipping of the chair.
Swivel
- Should enable the worker to easily rotate their body without rotating the spine or twisting the torso,
References
Bennett, C. L. (2001). Classroom sand Computers: An elementary school case study. Advances in Occupational Ergonomics and Safety, Vol. 4, 354-360.
Hedge, A., Barrero, M. and Maxwell, L., Ergonomic issues for classroom computing, In: Proceedings of the International Ergonomics Association and Human Factors and Ergonomic Society (IEA/HFES 2000), Human Factors and Ergonomic Society, Santa Monica, CA, 2000
Shinn, H., Romaine, K., Casimano, T and Jacobs, K. (2002). The effectiveness of ergonomic intervention in the classroom. Work, 18(1) 67-73.
Straker, L., Harris, C., Zandvliet, D., Scarring a generation of school children through poor introduction of information technology in schools, In: Proceedings of the International Ergonomics Association and Human Factors and Ergonomic Society (IEA/HFES 2000), Human Factors and Ergonomic Society, Santa Monica, CA, 2000
Williams, I.M., Computer ergonomic for teachers and students In: Proceedings of the International Ergonomics Association and Human Factors and Ergonomic Society (IEA/HFES 2000), Human Factors and Ergonomic Society, Santa Monica, CA, 2000
Anchel J. R., Kids and Computers: Eyes and Visual Systems, www.cvconsulting.com
School ergonomics programs, Cornell University Ergonomic Web, http://ergo.human.cornell.edu
Guidelines for Parents, Cornell University Ergonomic Web, http://ergo.human.cornell.edu
To Top
Lateral Epicondylitis (Tennis Elbow): Is There Any Science Out There?
By Jennifer Enns, Associate Ergonomist CCPE, MSc. Candidate, University of Waterloo
Lateral epicondylitis (LE) is a common upper extremity musculoskeletal disorder that is very problematic and has been reported to be an occupational risk for workers exposed to significant upper-limb stress (Kurppa et al., 1991; Viikari-Juntura et al, 1991), but yet it is poorly understood. Extensive epidemiological research has found a strong, consistent relationship between many types of Work Related Musculoskeletal Disorders (WMSD) and workplace exposure (NIOSH, 1997; Hagberg et al. 1995). However, the association of occupational exposures with lateral epicondylitis has been contradictory with some reviews suggesting a lack of a causal relationship for epicondylitis (Hagberg et al., 1995; Stock, 1991). Nevertheless, evidence of a relationship between work factors and LE has been reported to be strongest when examining exposure of a combination of risk factors (e.g. Force, posture, repetition) (NIOSH, 1997).
Symptoms and diagnosis
Lateral epicondylitis, also known as tennis elbow or elbow tendonitis, is a common disorder of the upper extremity that has been widely researched but is not yet fully understood. Clinically, it usually manifests as pain and tenderness over the lateral epicondyle or in the common extensor tendon immediately distal to the epicondyle. The symptoms are exacerbated when the wrist and finger extensors are firmly palpated or loaded. Loading of this area can be completed via stretching and contraction during hand and wrist use, or during resisted extension of the wrist especially while the elbow is in extension. In addition, it has been found that LE affects hand and forearm strength and function.
Clinical diagnosis of LE is based on manual palpation of the lateral epicondyle and provocation tests. Pain near the lateral epicondyle and small tendon of origin of the forearm extensor muscles indicates a problem exists (Ranney, 1993).
Descriptive illustrations may be found at: http://www.handuniversity.com/topics.asp?Topic_ID=5
Etiology (Causal Factors)
While most authors agree that the etiology of LE is related to overexertion of the wrist extensor muscles, the precise nature of the abnormality is uncertain. Clinical observations of LE have revealed that the etiological factors associated with LE are:
- Golf and other racquet sports (Coonrad & Hooper,1973; Goldie, 1964)
- Direct trauma, either a direct blow to the lateral epicondyle or a sudden indirect strain, as by a pull or forceful elbow extension (Goldie, 1964).
- Overexertion connected with a certain new pattern of movements introduced at work (Goldie, 1964; Dimberg, 1987)
- Persistent repetitive extension of the arm (Cyriax, 1936)
- Sudden or continued muscular strain (Cyriax, 1963; Goldie, 1964)
- Use of the arm in the same activity for many years (Goldie, 1964)
- Repeated dorsiflexions of the hand or alternating pronations and supinations (Goldie, 1964; Cyriax, 1936)
- Strenuous or repeated extension of the arm (Goldie, 1964)
- Overexertion of the extensor muscles of the wrist due to gripping and twisting movements (Dimberg, 1987)
- Jobs rated as moderate to high for elbow stress (Dimberg, 1987)
- No cause found (Goldie, 1964; Dimberg, 1987)
Biological Mechanisms
Many biomechanical studies of the upper extremity have been conducted to further understand the causes of LE and provide a link between the physical activities that people do and the disorders they acquire. The mechanisms of repetitive deviated postures, sustained exertions, and eccentric tensile loading are possible causes of LE.
Repeated deviated postures
Repeated deviated upper extremity postures involving flexion/extension (bending) and supination/pronation (twisting) of wrist that generates loads in the forearm/elbow region has been proven to be an important risk factor in WMSD's and has been shown to alter grip force production (Hagberg et al., 1995; NIOSH, 1997). Studies have revealed that overexertion of the extensors may occur from repeated wrist dorsiflexion (extension), forearm supination and pronation, and elbow extension (O'Sullivan & Gallwey, 2002; Mogk & Keir, 2003; Briggs & Elliot, 1985). These deviated postures increase stress on the forearm musculoskeletal system, which may lead to LE or other repetitive strain injuries.
Sustained exertions
Sustained extensor activity has been reported to be problematic in gripping and other similar single force tasks. Studies have revealed that the wrist extensors act as prime movers in extension and that wrist stabilizers resist wrist torque during gripping and other manual tasks. The wrist extensors get fewer pauses, are more exposed to static load than the flexor muscles, are exposed to increased passive forces, and increased risk with vibration exposure (Snijders et al., 1987; Hagg et al., 1997; Wells, Moore & Ranney, 1992; Keir & Wells, 2002; Kihlberg, Attebrant, Gemne & Kjellberg, 1995; Keir et al., 1996). Co-contraction of the extensors and sustained exertions are a control strategy required to maintain body position and to hold tools and work objects (Hagberg et al., 1995). This low level continuous or repeated loading may lead to overexertion and fatigue of the wrist extensors, thus causing LE.
Eccentric tensile loading
A major cause of LE is thought to be eccentric movements and their resulting internal micro tears, because eccentric contractions have been proven to cause injury (Lieber et al., 1991). Eccentric exertions are contractions of a muscle while lengthening, such as when body resists movement of external load like lowering work objects and resisting torque reaction of power tools (Hagberg et al., 1995) and also during tennis backhand stroke (Riek et al., 1999). Therefore, it is suggested that very high tension levels in wrist extensor muscles (specifically ECRB) during eccentric tensile loading may be a causative factor in lateral epicondylitis (Friden & Lieber, 1994; Lieber et al., 1991).
Conclusion
Although a strong association with work and LE has not yet been demonstrated, it is likely that repetitive deviated postures, sustained exertions, and eccentric tensile loading can cause the overexertion of the wrist extensors producing pathological changes associated with lateral epicondylitis. Due to the lack of consensus on the pathology of LE, the disorder may be more appropriately referred to as Lateral Elbow Disorder.
References
Briggs,C.A. & Elliott,B.G. (1985) Lateral epicondylitis: A review of structures associated with tennis elbow. Anatomia Clinica, 7, 149-153.
Coonrad, R.W., & Hooper, W.R. (1973) Tennis elbow: Its course, natural history, conservative and surgical management. Journal of Bone and Joint Surgery, 55A, 1177-1182.
Cyriax, J.H. (1936) The pathology and treatment of tennis elbow. Journal of Bone and Joint Surgery, 18, 821-940.
Dimberg, L. (1987) The prevalence and causation of tennis elbow (lateral humreal epicondylitis) in a population of workers in an engineering industry. Ergonomics, 30(3), 573-580.
Friden, J., & Lieber, R.L. (1994) Physiologic consequences of surgical lengthening of extensor carpi radialis brevis muscle-tendon junction for tennis elbow. Journal of Hand Surgery (American), 19A(2), 269-274.
Goldie, I. (1964) Epicondylitis lateralis humeri: A pathogenetical study. Acta Chir. Scand., 339 (Supple), 1-119.
Hagberg, M., Silverstein, B., Wells, R., Smith, R., Carayon, Hendrick, H.P., Perusse, M., Kouinka, I. & Forcier, L. (eds). (1995) Work-related musculoskeletal disorders (WMSD): A handbook for prevention, Taylor and Francis, London.
Keir, P.J., Wells, R., & Ranney, D. (1996) Passive properties of the forearm musculature with reference to hand and finger postures. Clinical Biomechanics. 7(11), 401-407.
Keir, P.J., & Wells, R.P. (2002) The effect of typing posture on wrist extensor muscle loading. Human Factors, 44(3), 392-403.
Kihlberg, S., Attebrant, M., Gemne, G., & Kjelberg, A. (1995) Acute effects of vibration from a chipping hammer and a grinder on the hand-arm system. Occupational Environmental Medicine, 52, 731-737.
Kruashaar & Nirschl (1999) Current concepts review: Tendinosis of the elbow (Tennis elbow): Clinical features and findings of histological, immunhistochemical, and electron microscopy studies. The Journal of Bone and Joint Surgery, 81A(2), 259-278.
To Top